L3-L5 Discectomy (Lumbar Spine)
An L3-L5 discectomy is a neurosurgical procedure that involves the removal of herniated disc material that is compressing the nerve roots in the lumbar spine. It is often performed to relieve symptoms such as leg pain (sciatica), numbness, and weakness.
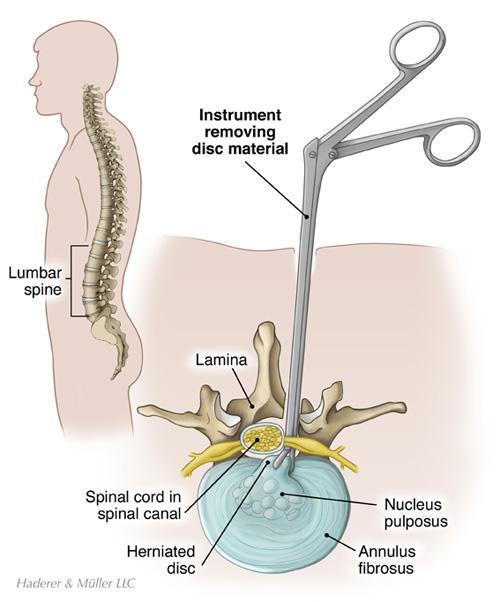
Relevant Anatomy
The procedure targets the intervertebral discs between the third and fifth lumbar vertebrae. Important structures include the dura mater, nerve roots, ligamentum flavum, facet joints, and paraspinal muscles.
1. Instruments and Equipment Checklist
Neuro Spine Tray (Sterile)
- Scalpel blades (No. 10, 15)
- Mayo and Metzenbaum scissors
- Adson and Debakey forceps
- Needle holders
- Kerrison rongeurs (1mm–5mm)
- Leksell and pituitary forceps
- Periosteal elevators (Cobb, Penfield)
- Laminectomy rongeurs
- Retractors (Taylor, Gelpi, McCulloch)
- Electrocautery (bovie)
- Suction (Frazier tip, Yankauer)
Specialised Equipment
- Operating microscope or loupes (surgeon preference)
- Microdiscectomy instruments
- Spinal curettes
- High-speed drill with fine burrs
- Neuro patties and cottonoids (x-ray detectable)
Sutures
- 3-0 or 4-0 Vicryl for deep closure
- 2-0 Nylon or staples for skin
Other Equipment
- Foam headrest or prone positioning frame (e.g. Wilson or Jackson table)
- Neuro pads and silicon gel pads
- Spinal drapes or major pack with drape extensions
- Sterile dressing (Opsite or Aquacel)
- Warming devices (Bair Hugger if required)
Fluids and Medications
- Antibiotics: Cefazolin IV pre-op as per facility policy
- Normal saline: For irrigation and flushing
- Local anaesthetic: Bupivacaine with adrenaline (if local infiltration used)
- TXA: Per anaesthetist/surgeon protocol (not always used)
2. Before Knife to Skin
- Ensure all instruments are counted and sterile field is complete
- Position patient prone with all pressure points protected
- Confirm spinal level with imaging prior to incision
- Apply electrocautery grounding pad and suction setup
- Coordinate with radiographer for intra-op X-ray or C-arm if used
Prepping and Draping
- Prep entire back region from T12 to sacrum with alcoholic chlorhexidine
- Drape using spinal drape pack or large extremity drapes, securing with towels
- Keep microscope covers sterile if used
3. Intraoperative Stages
- Incision: Midline lumbar incision over L3-L5 with bovie dissection to fascia
- Exposure: Dissection to expose lamina and facet joints using retractors
- Laminectomy: Bone removal with Kerrison or drill to access disc space
- Discectomy: Herniated disc material removed using pituitary forceps and curettes
- Haemostasis: Meticulously managed with bipolar cautery and surgicel
- Closure: Layered closure of fascia and subcutaneous layers, with skin staples or sutures
4. Post-Op Tasks
- Final count of swabs, sharps, and instruments
- Apply sterile dressing to wound site
- Assist with repositioning patient supine
- Dispose of sharps and clean instruments for reprocessing
- Document implants (if any), blood loss, and swab counts
- Handover to PACU staff with details of levels operated, blood loss, and any intra-op complications