Laparotomy for Small Bowel Resection and Stoma Formation
A laparotomy is a surgical procedure involving a large incision through the abdominal wall to access the abdominal cavity. This guide outlines the standard laparotomy approach for performing a small bowel resection and forming a stoma, commonly used for obstructed, ischemic, or perforated small intestine.
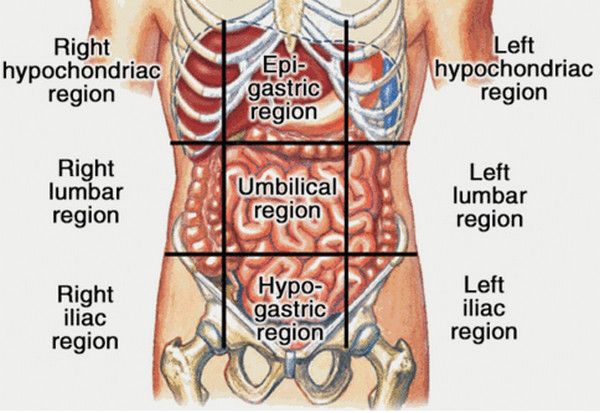
Relevant Anatomy
This procedure involves the peritoneum, small intestine (jejunum, ileum), mesentery, and potentially nearby organs such as the colon, omentum, and bladder. During stoma formation, the abdominal wall and skin are also surgically adapted for the bowel exteriorisation.
1. Instruments and Equipment Checklist
Basic Laparotomy Tray (Sterile)
- Scalpel blades (No. 10, 11, 15)
- Metzenbaum and Mayo scissors
- Tissue and dissecting forceps
- Needle holders
- Small and large retractors (Richardson, Deaver, Balfour)
- Suction tips (Yankauer and Poole)
- Debakey forceps, bowel clamps (Doyen), and haemostats
- Electrocautery (bovie)
Sutures
- Vicryl 2-0, 3-0
- PDS or Monocryl for bowel and fascial closure
- Nylon or staples for skin
Other Equipment
- Suction setup with sterile tubing
- Sterile bowls for irrigation (saline)
- Gauze, laparotomy pads
- Stoma rod (if required)
- Specimen containers
- Foley catheter and nasogastric tube (if required)
- Stoma appliance and wafer for marking or application
2. Before Knife to Skin
- Confirm patient consent for bowel resection and possible stoma
- Check and prepare all instruments and equipment
- Complete initial count of instruments and gauze
- Assist with prepping and draping the abdomen
- Stoma site marked by surgeon pre-op if planned
Patient Positioning
- Position: Supine
- Arms: Tucked or on armboards
- Padding: Pressure points protected
Skin Prepping and Draping
- Prep abdomen and planned stoma site
- Use alcoholic chlorhexidine or povidone-iodine
- Allow to dry fully before sterile draping
3. Intraoperative Stages
- Midline Incision: Open layers to enter peritoneal cavity
- Exploration: Inspect abdominal cavity, identify diseased bowel
- Mobilisation: Free affected small bowel segment and mesentery
- Small Bowel Resection: Apply Doyen clamps, divide bowel and mesentery, pass specimen
- Stoma Formation: Exteriorise proximal bowel loop through stoma site, mature as end or loop ileostomy
- Secure Stoma: Suture bowel to dermis, check viability and spout
- Check Haemostasis: Inspect resection site, mesentery, abdominal cavity
- Irrigation: Lavage with warm saline and suction clear
- Close Abdomen: Layered closure (peritoneum, fascia, subcut, skin)
4. Post-Op Tasks
- Final count of all instruments and gauze
- Ensure stoma is pink, moist, and patent
- Dress surgical wound and stoma site
- Complete documentation and specimen handling
- Assist with transfer to recovery or ICU as needed