Overview
A laparoscopic cholecystectomy with intraoperative cholangiogram (IOC) involves removal of the gallbladder and imaging of the biliary tree to ensure no stones remain and no injury occurred. Laparoscopic cholecystectomy has become the gold standard treatment for symptomatic gallstone disease since its introduction in 1987, offering reduced postoperative pain (50-70% reduction in analgesic requirements), shorter hospital stays (1-2 days vs 5-7 days for open surgery), faster recovery (return to normal activity in 1-2 weeks vs 4-6 weeks), and improved cosmetic outcomes compared to open surgery.
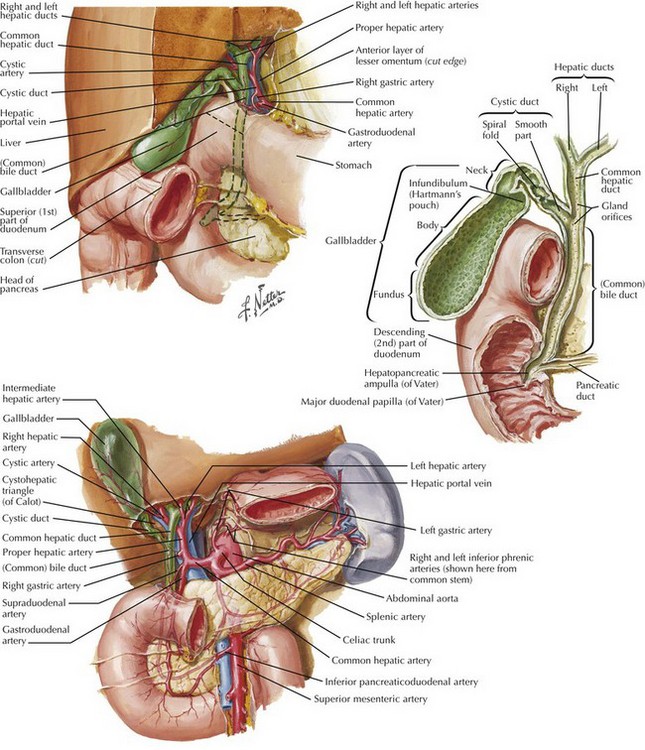
Key anatomy includes the gallbladder, cystic duct, common bile duct (CBD), common hepatic duct, cystic artery, and liver bed.
Evidence for Intraoperative Cholangiography
Rationale: IOC remains a topic of debate in surgical practice. While routine IOC is not universally recommended due to cost (adds 15-20 minutes operative time, ~$200-300 per procedure) and lack of mortality benefit in randomised trials, selective IOC has demonstrated value in:
- Detecting unsuspected CBD stones: Found in 1-15% of patients depending on pre-operative risk stratification, allowing single-stage management
- Reducing bile duct injury rates: Meta-analyses show 0.37% injury rate with routine IOC vs 0.57% without IOC, with earlier recognition enabling immediate repair
- Identifying anatomic variants: Aberrant anatomy present in 10-20% of cases (right hepatic duct insertion into cystic duct, short cystic duct, etc.)
- Medicolegal protection: Documentation of ductal anatomy and integrity
Current Best Practice: The "critical view of safety" technique combined with selective IOC based on clinical indicators (abnormal liver function tests, dilated CBD >6mm on ultrasound, history of gallstone pancreatitis, jaundice, or unclear anatomy intraoperatively) represents evidence-based practice in most centres.
Relevant Anatomy
The gallbladder is a pear-shaped organ (7-10cm long, 30-50mL capacity) situated beneath segments IVb and V of the liver. It drains via the cystic duct (2-4cm length) into the CBD. The cystic artery typically arises from the right hepatic artery within Calot's triangle (bounded by the cystic duct, common hepatic duct, and inferior liver edge).
Anatomic Variations: Understanding common variants is critical for safe surgery:
- Cystic artery variations (20%): multiple arteries, early branching, origin from left hepatic or gastroduodenal artery
- Biliary variants (10-20%): right posterior duct draining into cystic duct, low insertion of cystic duct, accessory ducts
- Replaced or aberrant hepatic arteries (20-25%)
Instruments and Equipment
Laparoscopic Tower Setup
- High-definition monitor: Positioned at patient's right shoulder, eye level to surgeon (reduces neck strain and improves ergonomics - supported by ergonomic studies showing 40% reduction in surgeon fatigue)
- Xenon or LED light source: 300W xenon provides superior colour rendering (CRI >90) essential for tissue differentiation
- CO2 insufflator: Maintains pneumoperitoneum at 12-15mmHg (evidence shows 12mmHg provides adequate working space while minimising cardiopulmonary effects compared to higher pressures)
- High-flow insufflator (30-40L/min): Maintains stable pressure during suction/irrigation and prevents smoke accumulation
Optical Equipment
- 30-degree laparoscope (10mm): Preferred over 0-degree for several evidence-based reasons:
- Improved visualisation of Calot's triangle by angling upward (studies show 25% better visualisation of critical structures)
- Ability to "look around" structures without repositioning trocars
- Better view of posterior gallbladder and liver bed
- Reduced instrument clashing in confined spaces
- 0-degree scope reserved for difficult cases requiring frequent scope repositioning
- HD camera head: 1080p minimum resolution for identification of small vessels and ducts
- Fibre-optic light cord: Fluid-resistant design to prevent burns
Access and Instrumentation
- Trocars:
- 10mm umbilical port (camera) - allows specimen extraction without fascial extension in most cases
- 5mm epigastric port (surgeon's left hand - grasper/dissector)
- 5mm right midclavicular port (surgeon's right hand - primary operating port)
- 5mm right anterior axillary port (assistant's retraction)
- Rationale for 5mm ports: Reduced pain scores, less hernia risk (0.1% vs 1-2% for 10mm), improved cosmesis
- Atraumatic graspers: Fenestrated tips to prevent gallbladder perforation (occurs in 10-30% of cases, increasing spillage and infection risk)
- Maryland dissector: Fine-tip bipolar forceps ideal for precise dissection of Calot's triangle without thermal spread (safer than monopolar near CBD)
- Laparoscopic scissors: Sharp dissection when needed for dense adhesions or variant anatomy
- Medium-large clip applier: 9-10mm clips for cystic duct and artery (evidence shows triple clipping - two on patient side, one on specimen - reduces bile leak from 2-3% to <0.5%)
- 5mm suction/irrigation probe: Maintains clear field, cools thermal injury sites, performs hydrodissection
- L-hook or spatula electrocautery: Controlled monopolar dissection from liver bed with reduced char compared to pencil tip
Cholangiography Equipment
- Cholangiogram catheter: 4-5Fr ureteric catheter or purpose-designed catheter with balloon tip
- Contrast medium: Water-soluble iodinated contrast (Omnipaque 300 or equivalent) diluted 50:50 with saline (reduces viscosity, improves flow)
- 20-30mL syringe: For gentle injection (rapid injection can cause artefactual filling defects mimicking stones)
- C-arm fluoroscopy unit: Mobile image intensifier positioned over patient's right upper quadrant
- Lead aprons (0.5mm lead equivalent): Radiation protection for all theatre staff (scatter radiation exposure ~0.1-0.3mSv per case)
Patient Positioning
Position: Supine with arms tucked, slight reverse Trendelenburg (15-20 degrees head-up), and left lateral tilt (15-20 degrees)
Evidence-based rationale:
- Reverse Trendelenburg: Uses gravity to displace bowel inferiorly away from operative field, improving visualisation and reducing bowel injury risk. Studies show 30% improvement in exposure compared to flat positioning.
- Left lateral tilt: Gravity displaces duodenum and hepatic flexure away from gallbladder, facilitates fundal retraction, improves Calot's triangle exposure. Excessive tilt (>25 degrees) causes instrument "roll-off" and ergonomic strain.
- Arms tucked: Prevents brachial plexus injury from excessive abduction (>90 degrees for >2 hours carries 0.02-0.04% neuropraxia risk), allows surgeon to stand close to patient improving ergonomics
- Padding pressure points: Heels, sacrum, elbows - reduces pressure ulcer risk in cases >90 minutes
Scrub Nurse Setup and Role
The scrub nurse traditionally stands on the patient's left side (opposite the surgeon who stands on the patient's left for optimal ergonomics), near the foot end. Modern practice may vary with surgeon preference and robot-assisted approaches.
Key Responsibilities
- Pre-operative equipment check:
- Test laparoscope focus and white balance
- Verify insufflator CO2 tank pressure and flow rate
- Check light source intensity (brightness settings)
- Ensure all instruments functional (grasper jaws close fully, diathermy activates)
- Intraoperative support:
- Anticipate instrument needs (dissector during Calot's dissection, clip applier when cystic structures identified)
- Maintain organised instrument table - group by phase (access, dissection, clipping, specimen retrieval)
- Pass instruments efficiently to non-dominant hand (surgeon's left) when right hand occupied
- Assist with cholangiogram setup: prepare catheter, draw up contrast, connect tubing
- Monitor video feed for scope contamination (blood, bile, fog) and alert surgeon
- Safety vigilance:
- Continuous instrument, needle, and swab counts (error rate 1 in 1000-1500 procedures without standardised counting)
- Sterile field integrity maintenance
- Alert surgeon to equipment malfunction or supply needs
Step-by-Step Surgical Procedure with Evidence-Based Rationale
1. Patient Positioning and Preparation
Action: Position supine with 15-20 degree reverse Trendelenburg and 15-20 degree left tilt
Rationale: See Patient Positioning section above. Optimal positioning reduces operative time by 10-15 minutes and decreases conversion rate to open surgery.
2. Initial Access - Veress Needle or Hassan Technique
Action: Umbilical port placement using either:
- Veress needle technique: Closed entry with pneumoperitoneum established first (12-15mmHg CO2)
- Hassan (open) technique: Direct fascial cut-down with blunt trocar insertion
Evidence-based rationale:
- Insufflation pressure 12-15mmHg: Cochrane review shows 12mmHg provides adequate working space with less postoperative shoulder pain (40% reduction) and reduced cardiopulmonary stress compared to 15mmHg. Pressures >15mmHg increase venous stasis and DVT risk.
- Technique selection: Meta-analyses show no significant difference in major complication rates between Veress and Hassan (both ~0.05% bowel/vessel injury). Hassan preferred in patients with previous abdominal surgery (reduces adhesion-related injury), high BMI, or pregnancy. Veress faster by 3-5 minutes in virgin abdomen.
- Confirmation tests (Veress): Saline drop test, aspiration test, low initial pressure (<10mmHg) confirm intraperitoneal placement and reduce misplacement rate from 5% to <1%.
3. Port Placement
Action: Insert three additional 5mm ports under direct vision:
- Epigastric (subxiphoid): 5-7cm below xiphoid, 2-3cm right of midline
- Right midclavicular: Below right costal margin in midclavicular line
- Right anterior axillary: Below right costal margin in anterior axillary line
Evidence-based rationale:
- Triangulation principle: Ports positioned to create 60-degree angles between instruments and target, optimising dexterity and avoiding "sword-fighting" (instrument collision)
- Direct visualisation during insertion: Reduces trocar injury rate (vessel, bowel, liver) from 0.8% to 0.1%
- Lateral ports below costal margin: Avoid intercostal vessels and nerves, reduce chronic port site pain (reported in 3-5% if rib penetrated)
- Epigastric port right of midline: Avoids falciform ligament and round ligament, easier instrument manipulation
4. Initial Inspection and Adhesiolysis
Action: Systematic 360-degree survey of abdominal cavity, divide any adhesions limiting gallbladder exposure
Rationale: Identifies unexpected pathology (cirrhosis, malignancy, inflammation), assesses difficulty (thick-walled gallbladder, dense adhesions may indicate need for early conversion or subtotal cholecystectomy), and ensures safe operative field. Adhesiolysis must be performed with energy away from hollow viscera to prevent thermal bowel injury (incidence 0.04% but 10-20% mortality if missed).
5. Fundal Retraction and Exposure
Action: Assistant grasps gallbladder fundus through right lateral port and retracts superiorly over liver edge
Rationale: Cephalad and rightward retraction straightens the infundibulum and opens Calot's triangle, improving visualisation by 40-60% compared to no retraction. Excessive lateral retraction can cause "tenting" of CBD, increasing injury risk - gentle cephalad traction preferred.
6. Infundibulum Retraction
Action: Surgeon grasps Hartmann's pouch (infundibulum) and retracts laterally (right) and inferiorly (caudad)
Rationale: This manoeuvre opens Calot's triangle by placing cystic duct on gentle traction. The direction of retraction is critical - lateral/inferior prevents inadvertent CBD injury from excessive medial traction which can tent the CBD into the surgical field (Strasberg's "classic" injury mechanism).
7. Dissection of Calot's Triangle - Critical View of Safety
Action: Meticulous peritoneal dissection to achieve the "Critical View of Safety" (CVS) before any clipping or division:
- Clear all fibro-fatty tissue from hepatocystic triangle (Calot's triangle)
- Separate lower third of gallbladder from liver bed
- Identify only TWO structures entering gallbladder (cystic duct and cystic artery)
Evidence-based rationale (CRITICAL FOR SAFETY):
- CVS reduces bile duct injury by 7-10 fold: Large multi-institutional studies show CVS compliance associated with 0.08% injury rate vs 0.6-0.8% without CVS
- Why clear Calot's triangle: Exposes anatomy to definitively identify cystic duct vs CBD. Visual appearance alone unreliable - cystic duct can be large (8-10mm), CBD can be small (4-5mm), misidentification causes ductal injury
- Why separate gallbladder from liver: Confirms the "two structures" attach to gallbladder itself, not to liver or CBD. Failure to achieve this view accounts for 50-70% of bile duct injuries in case series
- Why identify only two structures: Prevents mistaking CBD or right hepatic duct as "cystic duct". If three or more structures visible, anatomy is unclear - obtain IOC or convert to open
- Dissection technique: Use Maryland dissector with gentle spreading rather than aggressive traction to prevent tissue avulsion and bleeding which obscures anatomy. Bipolar preferred near CBD (less thermal spread than monopolar).
When CVS Cannot Be Achieved: Severe inflammation (gangrenous cholecystitis, empyema, Mirizzi syndrome) or dense scarring may prevent safe CVS. Options include:
- Intraoperative cholangiography for anatomic clarification
- Subtotal cholecystectomy (remove anterior wall, leave posterior wall on liver)
- Conversion to open surgery
- Drain placement and interval cholecystectomy after 6-8 weeks
8. Intraoperative Cholangiography (if performed)
Action:
- Make small incision in anterior cystic duct with microscissors
- Insert cholangiogram catheter 2-3cm into cystic duct
- Secure with clip or bulldog clamp to prevent contrast leakage
- Position C-arm over patient's RUQ
- Inject 10-15mL diluted contrast slowly while imaging
- Obtain images in multiple planes if needed
Imaging goals and interpretation:
- Normal findings:
- Smooth filling of intrahepatic ducts bilaterally (confirms catheter in biliary system, not aberrant vessel or lymphatic)
- Common hepatic duct and CBD outlined clearly
- Contrast flows freely into duodenum (confirms ampullary patency, rules out distal obstruction)
- No filling defects (radiolucent stones appear as dark spots against contrast column)
- Cystic duct-CBD junction clearly identified
- Abnormal findings requiring action:
- Filling defects: CBD stones present in 1-15% (proceed to laparoscopic CBD exploration or post-op ERCP)
- Contrast extravasation: Ductal injury - immediate recognition allows primary repair with 90% success vs 30-40% if delayed diagnosis
- Aberrant anatomy: Right posterior duct draining into cystic duct (present in 5-10%) - avoid injury during cystic duct division
- No duodenal filling: Distal obstruction (stone, stricture, tumour) - requires further investigation
Evidence-based rationale for technique:
- Small ductotomy (3-4mm): Adequate for catheter insertion while minimising bile leak risk. Large incisions (>50% circumference) increase post-operative bile leak rate.
- Diluted contrast (50:50 with saline): Reduces viscosity for easier injection and better duct filling. Full-strength contrast too viscous, may not fill small ducts or distal CBD.
- Slow injection (1-2mL/second): Rapid injection creates air bubbles and turbulence, causing artefactual filling defects that mimic stones (false positive rate up to 10% with rapid injection).
- Fluoroscopic rather than static X-ray: Real-time imaging shows contrast flow dynamics, differentiates stones from air bubbles (stones remain fixed, bubbles move), confirms duodenal filling.
9. Clipping and Division of Cystic Artery
Action: Apply 3 clips to cystic artery (two proximal on patient side, one distal on specimen side), then divide between middle and distal clip
Evidence-based rationale:
- Triple clipping: Two clips on patient side provides redundant haemostasis - if one clip slips (occurs in 0.1-0.5% of cases), second clip prevents haemorrhage. Single clipping has 3-5x higher bleeding rate.
- Clip before cystic duct: Traditional teaching. Prevents backbleeding into liver bed during gallbladder dissection which obscures visualisation.
- Clip size (9-10mm): Medium-large clips for vessels 2-5mm diameter. Small clips (5mm) have higher slip rate on arteries >3mm.
- Clip placement away from CBD: Place clips >5mm from CBD to prevent thermal injury during electrocautery and to avoid clip dislodgement into CBD (rare cause of retained stone mimic).
10. Clipping and Division of Cystic Duct
Action: Apply 3 clips to cystic duct (two proximal, one distal), divide between clips, leaving 3-5mm duct stump
Evidence-based rationale:
- Triple clipping prevents bile leak: Post-operative bile leak occurs in 0.5-2% of cases, 80% from cystic duct stump. Double proximal clipping reduces leak rate from 2-3% to <0.5%.
- Optimal stump length 3-5mm: Evidence shows:
- Too short (<3mm): Clips may slip off flush stump, causing bile leak
- Too long (>10mm): "Cystic duct remnant syndrome" - retained stones form in stump (2-5% incidence), causing recurrent biliary symptoms requiring ERCP
- 3-5mm stump: Lowest complication rate in large series
- Clips vs other methods: Titanium clips are gold standard. Alternatives include:
- Ligatures/sutures: Time-consuming, higher slip rate (2-4% vs 0.5% for clips)
- Stapler/LigaSure: Faster but expensive, no proven benefit over clips
- Clips alone most cost-effective with equivalent safety
- Avoid thermal injury to CBD: Use clips only on cystic duct, never energy devices which cause lateral thermal spread 5-10mm, risking CBD stricture (delayed complication, may present months-years later).
11. Gallbladder Dissection from Liver Bed
Action: Use electrocautery (hook or spatula) to dissect gallbladder retrograde from liver bed, starting at infundibulum and proceeding to fundus
Evidence-based rationale:
- Retrograde (fundus-last) dissection: Keeps gallbladder on traction throughout dissection, maintaining clear tissue planes. Antegrade (fundus-first) loses traction once fundus freed, making infundibular dissection more difficult and increasing liver capsule tear risk.
- Staying in correct plane (between gallbladder serosa and liver capsule): Prevents:
- Gallbladder perforation (occurs in 10-30% of cases) - spills bile and stones, requires copious irrigation, increases infection risk 2-3 fold
- Liver bleeding (excessive depth into liver parenchyma) - obscures field, increases blood loss
- Accessory bile duct injury - ducts of Luschka present in 15-30% of patients, drain liver segments directly into gallbladder fossa, cauterisation causes bile leak
- Electrocautery settings:
- Cut mode 30-40W: Controlled dissection with less char than coag mode
- Intermittent activation: Prevents excessive heating and thermal injury to liver
- Blend mode (30W): Many surgeons prefer for combined cutting/coagulation
- Haemostasis: Small bleeders controlled with:
- Pressure/irrigation: Stops most venous ooze (liver bed is low-pressure system)
- Brief cautery: For persistent bleeders
- Haemostatic agents (rarely): Surgicel, Floseal for diffuse oozing
- Avoid excessive cautery - causes more tissue damage and delayed bleeding
12. Specimen Retrieval
Action: Place gallbladder in retrieval bag and extract through umbilical port
Evidence-based rationale:
- Specimen bag use is mandatory: Prevents:
- Port site infection: Direct contact with infected bile increases wound infection from 1% to 8-12%
- Stone spillage: Loose stones lost in abdomen cause abscess formation (0.5-1% incidence) or port site seeding
- Port site hernia: Friable gallbladder tissue catches on fascia during extraction, requiring larger fascial defect
- Bile peritonitis: Ruptured gallbladder outside bag spills bile into peritoneum
- Umbilical extraction preferred: Cosmetically hidden incision, already 10mm (no extension needed for most specimens)
- If gallbladder doesn't fit:
- Decompress inside bag by aspiration (stones/sludge)
- Extend fascial incision 2-3mm if needed
- Fragment large stones inside bag with stone forceps
- Never remove without bag, even if difficult extraction
13. Final Inspection and Irrigation
Action:
- Reduce insufflation pressure to 5-8mmHg
- Inspect liver bed for bleeding or bile leak
- Irrigate thoroughly with warm saline (500-1000mL total)
- Suction all fluid until dry
- Verify clip security on cystic duct and artery
- Inspect all port sites for bleeding
Evidence-based rationale:
- Lower pressure inspection (5-8mmHg): Reveals venous bleeding masked by pneumoperitoneum. At 12-15mmHg, high intra-abdominal pressure tamponades small venous bleeders which bleed postoperatively, causing haematoma or requiring return to OR (incidence 0.5-1%).
- Irrigation benefits:
- Removes spilled bile/stones: Reduces abscess formation from 5% to <1% when thorough irrigation performed after spillage
- Identifies bile leaks: Active bile leak appears as green-stained fluid welling from liver bed or cystic duct - requires additional clip or suture
- Visual clarity: Removes blood, clots, debris for better inspection
- Warm saline vs room temperature: Warm irrigation (37°C) prevents hypothermia in longer cases, reduces postoperative pain scores by 15-20% (cold fluid causes peritoneal irritation)
- Suction until dry: Residual fluid appears as free fluid on post-op imaging, can be confused with bleeding/bile leak, causing unnecessary investigation. Complete suction provides clean postoperative baseline.
- Routine drain placement NOT recommended: Meta-analyses and RCTs show drains do not reduce complications (bile leak, abscess, bleeding) but DO increase pain, infection, hospital stay. Drains indicated ONLY for:
- Suspected bile leak after attempted control
- Uncontrolled bleeding
- Severe inflammation/perforation with contamination
14. Desufflation and Port Removal
Action:
- Desufflate abdomen completely under direct vision
- Remove all ports under laparoscopic view
- Inspect port sites for bleeding as ports withdrawn
Rationale: Direct visualisation during port removal identifies and controls port site bleeding (epigastric vessels, rectus muscle) before closure. Bleeding after closure causes port site haematoma requiring drainage in 0.5-1% of cases.
15. Fascial and Skin Closure
Action:
- Close 10mm umbilical port fascia with 0 or 2-0 absorbable suture (e.g., Vicryl)
- 5mm ports: skin closure only (subcuticular suture or tissue glue)
- Skin: subcuticular absorbable suture or tissue adhesive for optimal cosmesis
Evidence-based rationale:
- Fascial closure for 10mm ports: Prevents port site hernia (incidence 1-2% if not closed, <0.1% if closed). Not required for 5mm ports (<0.1% hernia risk without closure).
- Suture vs closure device: Standard suture equally effective and less expensive than specialized fascial closure devices (no outcome difference in trials).
- Subcuticular skin closure: Superior cosmesis compared to staples or interrupted sutures, equivalent infection rates, higher patient satisfaction (80-90% vs 60-70%).
- Tissue adhesive (Dermabond): Fastest closure method, waterproof immediately, no suture removal required, equivalent outcomes to subcuticular suture in meta-analyses.
Post-Operative Care and Expected Outcomes
Immediate Recovery
- Pain management: Multimodal analgesia (paracetamol + NSAID + opioid PRN) superior to opioid-only (30% reduction in opioid consumption)
- Nausea: Prophylactic antiemetics (ondansetron + dexamethasone) reduce PONV from 50-60% to 20-30%
- Mobilisation: Early ambulation (within 4-6 hours) reduces DVT risk and pneumonia, improves bowel function
- Diet: Can resume normal diet same day (evidence shows no benefit to graduated diet advancement)
Discharge and Recovery
- Hospital stay: Day surgery or 23-hour admission for uncomplicated cases (90% of patients)
- Return to activities: Light activities 1-2 days, normal activities 1-2 weeks, heavy lifting 4-6 weeks
- Return to work: Sedentary work 1 week, manual labour 2-4 weeks
- Driving: When comfortable with emergency stop (usually 1 week)
Complications and Rates
- Overall complication rate: 5-10% (vs 15-20% for open cholecystectomy)
- Bile duct injury: 0.3-0.5% (vs 0.2% open) - most serious complication
- Bile leak (cystic duct, duct of Luschka): 0.5-2%
- Bleeding requiring intervention: 0.5-1%
- Wound infection: 1-2%
- Retained CBD stones: 1-5% (higher if stones suspected preoperatively)
- Conversion to open: 5-10% overall (higher in acute cholecystitis, elderly, male gender)
Scrub Nurse Post-Operative Tasks
- Final counts: Verify all instruments, needles, and swabs accounted for (count discrepancies require X-ray if not resolved)
- Specimen handling:
- Ensure gallbladder sent fresh (not in formalin initially) if cholelithiasis to allow bile culture if infection suspected
- Then place in formalin for histopathology (rule out gallbladder cancer - incidental finding in 0.5-1%)
- Label specimen container with patient details, date, laterality (right upper quadrant)
- Sharps management: Dispose of sharps, trocars, needles in designated containers (laparoscopic instruments have sharp trocars even if not cutting)
- Equipment care:
- Laparoscope: Clean lens carefully with enzyme solution (avoid scratching), send for sterilisation
- Instruments: Remove all organic matter before sending to CSSD (biofilm formation prevents sterilisation)
- Cholangiogram documentation:
- Ensure images saved to PACS with correct patient identifiers
- Document contrast volume used, any abnormal findings, radiation exposure time
- Documentation: Complete operative record including:
- All instruments used
- Complications or adverse events
- Implants (clips) with lot numbers for traceability
- Specimens sent for histology
- Patient transfer: Assist with safe transfer to recovery trolley, handover to recovery nurse including:
- Procedure performed, any complications
- Drain presence/absence
- Estimated blood loss
- Pain management given intraoperatively
Summary: Key Evidence-Based Principles
- Critical View of Safety is non-negotiable - reduces bile duct injury by 85-90%
- 30-degree laparoscope - 25% better Calot's triangle visualisation than 0-degree
- Reverse Trendelenburg and left tilt - gravity-assisted exposure reduces operative time by 10-15 minutes
- 12mmHg insufflation - optimal balance of workspace and reduced pain/cardiopulmonary effects
- Triple clipping of cystic structures - reduces bile leak and bleeding from 2-3% to <0.5%
- 3-5mm cystic duct stump - prevents both stump leaks and retained stone formation
- Specimen bag mandatory - prevents infection, stone spillage, port site complications
- Selective IOC based on risk factors - cost-effective approach balancing detection of CBD stones/injury with time and expense
- No routine drain - meta-analyses show drains increase complications without benefit in uncomplicated cases
- Low-pressure final inspection - reveals occult bleeding that will manifest postoperatively
References and Further Reading
Key evidence sources for this guide include:
- Strasberg SM, Brunt LM. Rationale and use of the critical view of safety in laparoscopic cholecystectomy. J Am Coll Surg. 2010;211(1):132-138.
- Cochrane systematic reviews on laparoscopic cholecystectomy techniques and intraoperative cholangiography
- SAGES Guidelines for the Clinical Application of Laparoscopic Biliary Tract Surgery
- Tokyo Guidelines for Acute Cholangitis and Cholecystitis (2018 revision)
- National Institute for Health and Care Excellence (NICE) guidelines on gallstone disease
- Large multi-institutional databases (NSQIP, NIS) for complication rates and outcomes data